Can a smart digital assistant with 3-D vision help improve musculoskeletal care?
Today's musculoskeletal care exists along a spectrum, with watchful waiting at one end (hoping a muscle strain or bruise simply resolves), and surgical repair of broken or torn bones, ligaments, or muscles at the other. And at every point along the spectrum, there can be a role for professional physical therapy, most often inclusive of directed, home-based exercise programs to aid in recovery from surgery or injury. Effective management of home-based therapeutic exercise poses many challenges, starting at whether patients understand what is expected of them, including whether they can effectively perform and complete their prescribed activities, whether their reporting of their performance is accurate, and finally whether less than desired progress represents a failure of the prescription, a failure of adherence, or some other misunderstanding. These and other frustrations encourage therapists to see their patients more often to reinforce teaching and trainings and assess interval progress.
What if there was a smart home assistant to educate, instruct, remind, measure, monitor, record and provide audio-visual feedback on each patient's performance. Would such an aid make it possible for patients to progress with less frequent in-person check-ins? Would patients use it? Would it aid adherence? Would it save money? These are the questions we set out to answer a few years ago, and after building a company to make such a thing, deploying it, studying it, and watching patient and clinician reaction, I believe the answer is an affirmative yes to all.
To briefly recap: Years ago, the advent of low-cost, high quality 3-D cameras provided a technology platform for quantifying human posture and pose. We imagined adding an engaging multilingual avatar for patient instruction, a comprehensive analytic back-end, and a clinical dashboard for rapid review, oversight, and tailoring of rehabilitation prescription for each patient by expert clinicians. By doing this all free from the constraints of synchronizing patient and provider schedules or location, it seemed intuitively obvious that one could dramatically improve the post-acute care recovery process for everyone involved.
And so, that is what we did.
We built VERA(TM), a Virtual Exercise Rehabilitation Assistant, an interactive avatar for helping patients with their rehabilitative exercise programs. We made her engaging, and we proved this out by testing various candidate personas with focus groups and choosing our avatar from a sea of also-rans to that we could maximize engagement.
We taught VERA how to instruct patients on the appropriate way to perform hundreds of therapeutic exercises, and we taught her how to demonstrate such exercises so that patients could see and better understand what was being asked of them.
We gave VERA 3-D vision - so that she could measure joint positions and calculate joint angles and limb velocities 30 times each second. We asked VERA to keep track of patient's movements in the context of specific instructed movements, and we taught her to count repetitions of desired movement and make notations when the movements strayed from the instructed movement. We enabled VERA to give audio-visual feedback to patients as they performed their instructed movements, reinforcing to the patients that they were being watched. And we recorded everything so that expert clinicians could review off-line.
And we built in the opportunity for 3-way televisits between the patient, their clinician and all of VERA's compiled measurements and video recordings.
And then we tested VERA -- really tested VERA - in a large, prospective, randomized, controlled trial of patients undergoing knee replacement. The control group received the best standard of care, typical, in-person, face-to-face time with expert therapists and at-home exercise programs in between the face-to-face visits. The intervention group received VERA in their home. VERA provided education and instruction, taking them through their prescribed regimen. VERA measured and monitored and catalogued their performance, all under the guidance of the same therapists providing face-to-face care in the control group.
It was as balanced and thoughtful a trial as we could conduct. And -- importantly, we didn't conduct the trial ourselves. Rather, we commissioned the largest and best regarded academic clinical research organization in the US to help design and then conduct the trial for us --DCRI (Duke Clinical Research Institute), with Janet Prvu Bettger, ScD as the independent principal investigator, and enrolled patients from both academic as well as private practice settings.
2 Years and millions of dollars later, we were presented with the results.
First, patients liked and could easily use VERA. This was no surprise to us as using VERA decreases the need for travel (back and forth to therapists' office) and copays. And our routinely collected net promoter scores (NPS) - a measure of whether you would tell your friend to use it, always exceeded those of Apple products and Amazon services.
Patients used it -- patients exercised with VERA an average of 5.9 days each week and 26 minutes each day!
And, In the vernacular of clinical trials, the entire cohort of patients who worked with VERA had objective clinical outcomes that were "non-inferior" to those achieved by patients in the control, in-person, face-to-face group. The data has been presented in abstract form, and the full manuscript has been submitted to The Journal of Bone and Joint Surgery.
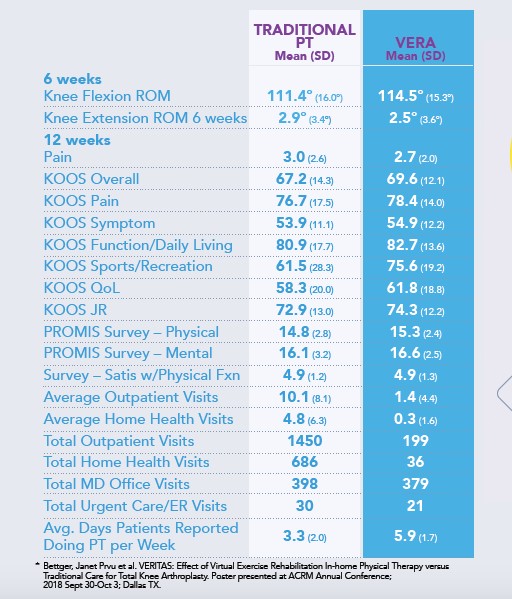
The VERA group was superior in nearly every metric, though that wasn't the primary question that the trial asked. And when we looked a little deeper at an outcome that patients and surgeons alike really care about, that being the number of patients left with severe or extreme limitations in activities of daily living at the end of 3 months. We again saw that the VERA group had fewer such patients for 29 of 30 specific physical activities of daily living - and while this is a strikingly positive finding, this was also not a primary endpoint of the study.
We designed this trial primarily to capture overall healthcare spending, and the patients who worked with VERA had fewer encounters with the healthcare system (decreased re-admissions, decreased SNF stays, decreased ER visits, decreased home health visits, etc), with their total cost of care being $2745 less than control.
So, can a smart digital assistant help improve patient experience and outcomes (while simultaneously reducing cost) in musculoskeletal care? Yes. Absolutely.
And what is next? VERA's capabilities continue to be refined and extended, with additional clearance by the FDA to use the same methodology for the rest of the body, focusing on trunk (back) and upper extremity.
Smart assistants are in our phones, our homes, and our cars - and when used appropriately, they can help us find answers to our questions, order our food, find the nearest gas station, and even, as we have demonstrated, help us with our healthcare needs in a way that saves us all time, steps and money.
About the Author:
As the president and chief executive officer of Reflexion Health and Digital Health Corp, Dr. Joseph (Joe) Smith’s expertise and passion lies in exploring the intersection of medicine and technology. His background includes serving as the founding chief medical and science officer at the West Health Institute, president of the West Health Policy Center in Washington, D.C., and manager of the West Health Investment Fund. He has also held executive positions at J&J, Boston Scientific, and Guidant Corp. served as a practicing cardiologist for close to 20 years. Dr. Smith holds bachelor’s degree from Johns Hopkins, a PhD from MIT, and an MD from Harvard Medical School.